Guest Editorial by Estelle Ricoux, Co-founder, Design and Strategy Director at Firm
China has become the world’s most active source of early-stage oncology assets. And for most drug classes, in-licensing a promising molecule is a transaction. For Radioligand Therapy (RLT), it is only the beginning of the problem.
A radioactive drug must reach a patient within days of production. That requires not just a manufacturing site, but a licensed facility, a cold-chain distribution network, reimbursement architecture, and isotope supply; all functioning in concert. In markets like the US, these elements exist as separate, established industries. In China, most of them are still being built. The result is a market where the science is moving faster than the system designed to deliver it, and where the decisions a developer makes today about pathways, partners, and isotopes will shape whether their therapy ever reaches a patient at commercial scale.
Logistics vs infrastructure
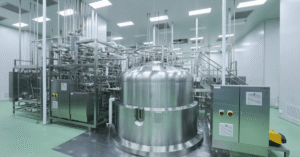
Currently, the ability to discover new molecules has outpaced physical infrastructure. A shortage of licensed facilities and specialized radiochemistry expertise makes it difficult for many companies to move beyond discovery into manufacturing.
In mature markets like the US, CDMOs can focus almost exclusively on manufacturing by relying on established nuclear pharmacy networks for distribution. China’s infrastructure presents a fundamentally different challenge. Because the market lacks a mature, decentralized pharmacy network, CDMOs must solve the “last-mile” delivery problem themselves.
To support commercialization, a provider must bridge the gap to the patient by building proprietary, integrated ground and air transport systems. Achieving the 24-72h delivery window required for RLT on a nationwide scale requires a level of infrastructure investment that most providers have yet to make.
Reimbursement architecture
Physical infrastructure is not the only barrier; the financial framework is also lagging. Currently, the National Reimbursement Drug List (NRDL) lacks a dedicated category for therapeutic radiopharmaceuticals, often leading insurance agencies to apply a “diagnostic-only” mindset when evaluating costs.
This results in a significant pricing challenge. The NRDL’s “Volume-for-Price” model typically caps the annual cost of reimbursable drugs at roughly 300,000 RMB (~$42k USD). For an innovative RLT, this often fails to cover a full cycle of therapy. While the new Commercial Insurance List aims to cover high-cost therapies outside the NRDL, the primary pathway for early access remains the hospital-led trial.
The choice that comes with the “Category 4” IIT pathway
In China, licensed hospitals can manufacture and administer unapproved drugs under Investigator-Initiated Trials (IITs, known as the Category 4 pathway). For Western companies, this is an efficient way to generate human data quickly, and accelerates the transition to Phase 1 or 2 trials in the US or in Europe.
However, this speed comes with a significant commercial risk when it comes to the path to commercialization in China. The issue is commonly misread, even by experienced Western teams. Chenchao Liu, Managing Director at SILREAL, explains:
“The Category 4 hospital manufacturing dynamic is often misread outside China. The core issue is not simply lower-cost hospital production, but how this interacts with China’s DRG/DIP payment reform and can create structural reimbursement ceilings before a product reaches NRDL negotiation. Many Western teams frame this as a pricing issue. In practice, it is a reimbursement architecture issue, and the strategic response differs materially depending on whether entry is built around an IIT pathway or a standard NDA route.”
A hospital manufacturing an RLT in-house under a fixed government payment structure has a strong financial incentive to continue doing so even after a commercial version launches. Not because it is cheaper, but because it fits within an existing reimbursement logic that the approved product may not. For a Western developer, this can establish a structural ceiling before national insurance negotiations even begin. The choice between the IIT pathway and a standard NDA route is not simply a question of speed versus rigour; it is a decision about what reimbursement architecture your commercial entry will be measured against.
The Isotope Supply Race
Chinese Radioligand Therapy R&D will only become globally competitive when domestic radionuclide supply is secured. Currently, ecosystems are not developing equally across isotopes. While domestic production of Lutetium-177 is maturing, the supply of alpha-emitters like Actinium-225 or Astatine-211 remains highly constrained and dependent on specialized cyclotron or generator capacity that is still being built.
To address this, companies like Alpha Nuclide are establishing decentralized, multi-site production networks. By building regional centers in Eastern China (Jiaxing) and Northern China (Shijiazhuang), they are creating an infrastructure designed to deliver the isotope on-demand to local clinical sites. For a developer, the choice of a radionuclide is no longer just a scientific decision; it is a strategic commitment to a specific, localized infrastructure network. Whichever nuclide becomes truly accessible and affordable first will dictate which clinical programs reach the market.
The “Agnostic” CDMO Challenge
Most Chinese RLT CDMOs currently boast superior facilities, data management plans, and capacities compared to many US or EU providers, largely due to recent, strict GMP-aligned infrastructure builds. However, a structural trap remains: different isotopes require different infrastructure and safety protocols, making it economically unviable to build a “universal” facility for every radionuclide.
This raises the question: can a “generalist” truly master the chemistry of every isotope? Charles Conroy, Managing Partner at Radion Advisory Group and former CEO of Nucleus RadioPharma, suggests that while an “isotope agnostic” label implies flexible equipment, it does not guarantee expertise. He notes that because every isotope behaves differently in radiochemistry, optimizing yield, stability, and scale-up still requires deep, isotope-specific knowledge. According to Conroy, the strongest CDMOs in this evolving market will be those that marry flexible infrastructure with teams that truly understand the unique chemistry challenges of each individual isotope.
The evidence from China suggests the answer is already emerging. In a market where isotope supply is fragmented, distribution requires proprietary infrastructure, and clinical timelines are compressed, generalist positioning is increasingly a liability. The CDMOs gaining traction are those building deep around a specific radionuclide: owning the supply chain, mastering the chemistry, and becoming the only logical choice for a developer working in that space. The “agnostic” label may remain useful as a sales posture, but as Conroy implies, the underlying reality will be specialists wearing a generalist’s coat. For developers evaluating partners, the sharper question is not “can this CDMO handle my isotope?” but “have they truly built around it?”
From vendor to strategic architect
To successfully enter the Chinese market, radiopharmaceutical companies must answer decisive questions at the intersection of regulatory pathways, reimbursement design, isotope supply, and hospital execution.
The complexity of the Chinese market serves as a magnifying glass for global RLT challenges. It demonstrates that for the developer, the core question has shifted from “Does this molecule work?” to “Can this molecule be delivered profitably within a fixed-payment architecture?”
This shift demands a new standard for the relationship between developer and CDMO. The future belongs to integrated partnerships, but integration means something specific here. It means a provider who has built deep technical mastery around a particular isotope rather than claiming fluency in all of them. It means owning the last mile, not subcontracting it. And it means arriving at the commercial conversation already fluent in the local reimbursement architecture, not learning it alongside the client.
That is what a strategic architect looks like, as distinct from a manufacturer. China has made the difference between the two impossible to ignore. In the next era of RLT, the infrastructure is not a support function for the innovation. It is the innovation.
Estelle Ricoux is Co-founder and Design & Strategy Director at Firm, a consultancy dedicated to accelerating the delivery of advanced therapies. With 20 years of experience at the intersection of human experience and complex systems, Estelle partners with pharmaceutical companies to design end-to-end service experiences and build the digital infrastructure required to deliver radioligand and other advanced therapies at scale.